Plaque Control, Dental Hygiene, and the
Pioneering Work of Charles C. Bass
Adam Blatner, M.D.
(This is an addendum to the six-lecture series
titled "Stories in the History of Medicine" given at the Senior
University Georgetown’s Winter-Spring 2009 session.)
To read other lectures in this series: Click on: 1. Introduction and Beginnings of Germ Theory. which also has, three supplements, which you can click on to link to related webpages:
A. A very brief overview of the history of medicine. (pre-history to the Renaissance) (just to get you oriented)
B. Further Overview to modern times.
C. A further history of microscopy.
Other lectures: 2: Contagion, Infection, Antisepsis ; 3: The Early History of Immunology ; 4: The Discovery of Anesthesia;
5: Recognizing Nutritional Deficiencies 6: Hygiene: Preventive Approaches to Cholera and Hookworm.
This present webpage: (Addendum: 6a: Dental Hygiene & Plaque Control) , Dental Hygiene
(First Posted March, 2009; Revised, expanded, re-posted: November 14, 2011)
To read other lectures in this series: Click on: 1. Introduction and Beginnings of Germ Theory. which also has, three supplements, which you can click on to link to related webpages:
A. A very brief overview of the history of medicine. (pre-history to the Renaissance) (just to get you oriented)
B. Further Overview to modern times.
C. A further history of microscopy.
Other lectures: 2: Contagion, Infection, Antisepsis ; 3: The Early History of Immunology ; 4: The Discovery of Anesthesia;
5: Recognizing Nutritional Deficiencies 6: Hygiene: Preventive Approaches to Cholera and Hookworm.
This present webpage: (Addendum: 6a: Dental Hygiene & Plaque Control) , Dental Hygiene
(First Posted March, 2009; Revised, expanded, re-posted: November 14, 2011)
"An ounce of prevention is worth a pound of
cure."
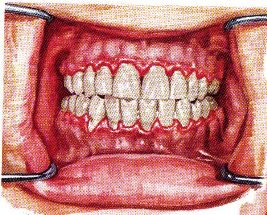
Most people past the age of 30 begin to have more obvious, symptomatic gum disease.
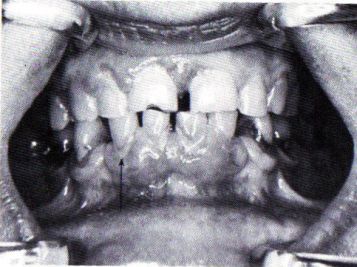 |
| Arrow points to dental plaque, associated
with swollen and reddened inflamed gums (gingivitis,
periodontitis). |
People born before around 1920 often began to suffer from toothache by their middle years; they often had the offending teeth pulled and it was common that people sought a partial or full set of dentures (false teeth) by the time they were in their 50s or 60s.
Not only was this pattern a source of chronic discomfort, acute episodes of pain, the financial strain of dental fees, the discomfort also of ill-fitting dentures, and so forth, but the loss of teeth or their tenderness led to dietary changes---a loss of heartier, chewier, food---sometimes favorite foods!---, and an increasing risk of nutritional deficiency. Nor whould we underestimate the subtle loss to the family and community that comes with a person who is in discomfort---grouchiness, embarrassment at smiling with teeth missing, a tendency not to smile, bad breath, and so forth. This problem also perpetuated age-ism, a subtle stereotype of toothless elderhood as less attractive, healthy, or vital.
In other words, I used to think most dental problems are due to cavities, a tooth problem; what's emerging is that most cavities are in turn caused by gum problems, even more so in adulthood. There is also mounting evidence that chronic inflammation is associated with low grade infection, and this in turn may be a factor in the formation of atherosclerosis, heart attacks, and other systemic medical problems. So it is worthwhile to seek ways of understanding and countering gum inflammation.
Only in the last fifty years have they elucidated the causes of this pervasive condition, and shown that reasonably easy techniques of regular flossing and brushing can prevent this condition! While some tooth decay is probably inevitable, much of it can be prevented.
Plaque Build-up: The Real Cause of Tooth Decay and Loss in Adulthood
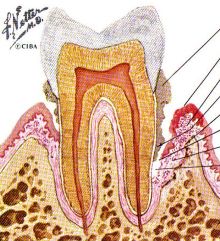 |
Also comparing the degeneration on the right as compared to the left, you'll notice the bone has shrunken, as chronic inflammation of the gum will dissolve bone, so there is a tendency to loosenses. You can see that the calculus goes down below the gum-line. The pocket is much deeper and the peridental membrane is vulnerable to infection and cavity-producing processes. More, the whole tooth is more vulnerable because the gums are swollen. The old joke, "Your teeth are okay but your gums will have to come out" (a line I heard around 1950) turns out to be kind of true! Not come out, but your gums are what need to be treated.
What they discovered about fifty years ago about the nature of dental plaque took about twenty years to get to the dentists and another 20 years to become mainstream with dental hygienists. Even so, it's not explained well: From my own informal research, less than ten per cent of people understand the actual reasons one should floss! , and most folks today still don’t know about it. Here is a cross-section, here’s the chronic inflammation, here’s where infection sets in and side-cavities, leading to deeper abcesses, the need for root canals, crowns, extractions.
 |
It took a good deal of time for the theory which I’ll be explaining to you more in a minute or two to get disseminated into the population. First, the biology of the condition needed to be explored. The main fellow who did this was not a dentist, but rather a physician. (Just as a dentist was a pioneer of anesthesia and surgery, so also can a physician be a pioneer of dentistry.). Interestingly, this physician, Charles C. Bass, M.D. (1875-1975), is the same fellow who was also a minor pioneer in hookworm research and treatment in the Southern USA, as noted in that earlier part of this lecture (and on that related webpage). Bass was on the faculty of the Tulane University Medical School in New Orleans, where he: (1) isolated the hookworm ova, and published Hookworm Diseases in 1909, with Dr. George Dock; (2) first identified beriberi and pellagra in Louisiana; (3) simplified the method of diagnosing typhoid fever; (4) discovered a method to cultivate the plasmodia organism, allowing malaria research as never before; (5) developed a rational theory for tooth decay based on the idea of plaque control; and (6) devised a practical nylon-based dental floss and worked out how to most effectively use it. This work was revised and refined further by a dentist, Dr. Sumter S. Arnim, DDS, and others.
 |
 |
Of course, tooth brushing has been around for literally thousands of years. But it doesn’t really do the job where it is needed, which is at the gum line. For that you need dental floss: A brief summary here: In 1815 a dentist named Levi Spear Parmly, also from New Orleans, first published a paper recommending flossing, at that time, with silk. The next advance was decades later, in 1892, when the Codman and Shurtleft Company manufactured human-usable unwaxed silk floss; and not long thereafter, in 1898, the Johnson & Johnson Corporation obtained the first patent for dental floss.
The next development was in the 1940s when Dr. Bass developed nylon floss, which was more resilient and stronger than silk.
 |
However, it wasn't until the late 1960s that the idea started becoming effectively disseminated: Plaque control via floss becoming more prevalent in dentistry. The next challenge is then to sell it to the dental hygeinists and then through them and the dentists, to sell it to the public. This is slow-going. Recently, survey shows only about 12 percent of Americans floss daily, 39 percent floss less than daily, and 49 percent do not floss at all.
To re-emphasize the theme of developing underlying technology: What's needed is a floss that is thin enough to get in between the teeth, but not so thin that it breaks easily, and smooth enough to slip and move. Floss wasn’t used much when it was cotton or silk. Technology again breaks through. Nylon not only makes cheaper ladies’ stockings, it makes a stronger and smoother floss!
The Biology of Dental Plaque
 |
 |
 |
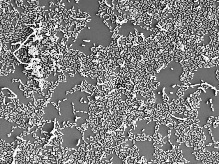
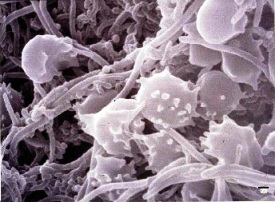
67 Let’s look at the nature of dental plaque, to see why flossing works.First of all, there are more germs in your mouth than there are people on the earth! (Leeuwenhoek made a similar claim, saying that there were more than all the men in the Netherlands! Big underestimation!) To the right are two picutres that first show the general biofil, and then with a scanning electron microscope, the peculiar "corncob" formation of the way some of these germs aggregate.
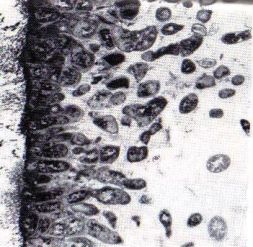 |
Bass and some others did careful research and discovered that plaque is not just a layer of germs that can be brushed off. First of all, not just one kind of germ is involved, but over a hundred different kinds! Here is a cross section (on the left, another electron microscope) of dental plaque against the trooth (again against the left).
This is explained more diagrammatically in the picture to the lower right:
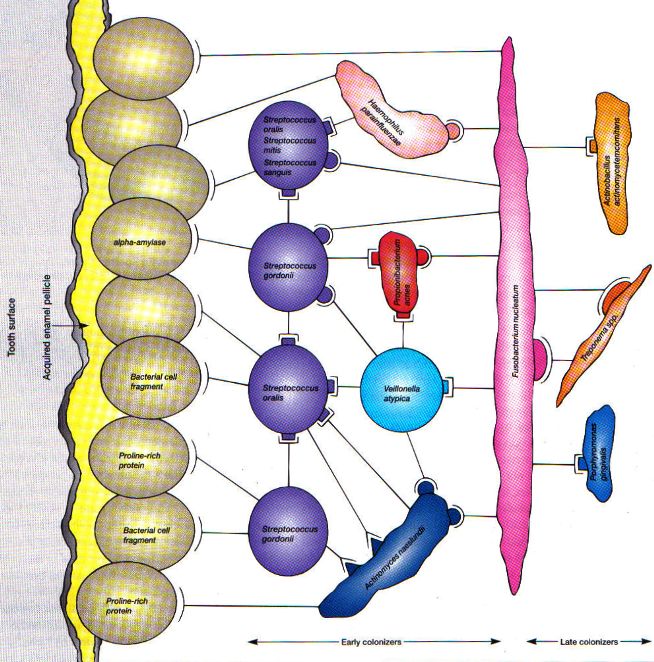 |
This is a very common germ. Hardly any of these are the type that give "strep throat" or rheumatic fever. And more, they alone don't make that much trouble. But they're sticky, and to them attach the other germs, sometimes other strains or species of streptococcus, forming that aforementioned "corncob" formation, and often other types. This whole process commences anew every time you brush your teeth, building up over twenty-four hours.
 |
See the little strands they put out? They're no longer nice little round germs minding their own business. You know how when nice kids get together they sometimes get pretty rowdy? And the lifeguard comes along and yells, "Okay, everybody out of the pool! and they all cool off and quiet down? Well, that's sort of what flossing does. The problem is the aggregate, their ecology, because from this aggregate they accumulate waste, just as we heard about with cholera or hookworm, only this is germ poop. It's acidic and it irritates the gums. If it's allowed to stick around, the gums react by becoming more and more inflamed.
 |
The trouble with this aggregate is that the germs near the bottom that need oxygen can't get enough; they die off; their rotting bodies are food for the other germ types that don't need oxygen---indeed, they can't stand the stuff!---they're called anerobicc bacteria, meaning without-air. This physiology is important, because if you can just get air into that pile of sticky germs that is dental plaque, you can break the cycle! That's where flossing comes in.
There are too many germs to get rid of them---you can use all the mouthwash in the world. The good news, though, is that you don't have to brush and floss after every meal. On the other hand, you do need to do it once every 24 hours---doesn't really matter whether it's morning or evening. If you delay, that give the build-up of irritating substances given off by the aggregate time to inflame the gums, which then leads to the other problems of gum and tooth breakdown.
How to Floss Correctly
Run the floss up and down along the gum line, especially between the teeth. The brush should also go up and down. A little cross-ways movement is okay, but not really needed, and too much cross-ways movement then abrades and injures the teeth and gums at that point. So mainly try to go up and down or gently in a circle. The goal is to remove some of the plaque, but mainly---this is the key---to break it up, allow oxygen in the air to penetrate down deep, kill the anerobes, and interrupt the ecological cycle that produces gum-irritating acid waste!(Most people have not had this explained to them by their dentist or dental hygienist!)
 |
Do not use this as an excuse to stop! Do not think, "Whoa! This must be bad for my gums!" You don't have to floss hard, but do it, break up that plaque, brush, let it bleed a bit. The irritating source is being removed! The gums will begin to heal. It will take about two to three weeks if you keep at it! Keep at it, every day (or at bedtime. My wife and I read to each other---one read while the other flosses). Gradually the gums will become less tender, the bleeding will lessen, and finally pain and bleeding will stop.
The pockets behind the gums will become shallower. Your dentist or dental hygienist will be pleased. (Tell them about this webpage!) Hang in there. Hold on to your teeth!
The healing is not from massaging the gums. And getting food particles from out between the teeth is not the therapeutic thing either, though it may help just a tiny bit.
 |
In the olden days occasionally they diagnosed "gingivitis" (gum infection), but most folks just thought it was the fault of the teeth getting rotten. The point of Bass' research, though, is that "common sense" is again mistaken. It's the gums that are the problem, especially right at the gum line—the plaque! So this gave a big boost to a new field, "periodontology," the study of the tissues around (para) the teeth (odont)!
Habit Development
Another reason I particularly enjoy this idea is because it is an example of how it takes time and patience to break an old habit, such as the habit of not brushing or flossing, and to build a new habit in its stead. Many of you know I'm a psychiatrist interested in mental hygiene---prevention---and part of that is to build habits of more positive and effective types of thinking that then supports the development of habits of more positive feeling, too.Acknowledgement: My wife, Allee Blatner, worked in a dental office in the early 1970s and taught me about Bass' work and how to floss correctly, stimulated my reading and got me excited about the way good dental hygiene can make a big difference in people's lives!)
References
Christen, A. (April, 1982). Charles C. Bass, M.D.--1875-1975: that cantankerous genius of preventive dentistry. Bulletin of the History of Dentistry, 30 (1).Lott, Wayne (with Steve Brawner). (2004). Dr. Charles Bass & the Bass Method: One man's crusade to end tooth decay and gum disease. Lincoln, NE: xLibris. (www.xlibris.com)
O'Hara, J. W. (October, 1991). Prevention revisited: Dr. Bass meets Dr. Robert F. Barkley. Bulletin of the History of Dentistry, 39 (2).
Addendum: From
Wilson, Michael. (2008). Chapter 8: The indigenous microbiota of the oral cavity. In: Bacteriology of Humans: An ecological perspective. Malden, MA (USA) and Oxford, UK: Blackwell.
Interesting photos and diagrams reinforcing points made above.